7.5 Estimating Protein Needs
The main factors that determine an individual’s need for protein are body weight and activity level. The DRI for protein for a sedentary adult is 0.8 g/kg of body weight per day. This is the minimum amount of protein needed to maintain body tissues and perform the primary functions of protein. Athletes and active individuals require between 1.2-2.0 g/kg, well above the minimum protein recommendations, to support physical activity and maintain muscle mass (1). Protein intakes greater than 2.0 g/kg/day are considered excessive and do not appear to offer any additional benefit to an athlete in terms of improved performance or muscle protein synthesis. Table 7.5 illustrates the variation in protein recommendations for different types of athletes.
Table 7.5 Protein Requirement by Activity Level
| Level of Activity | Protein requirement in g/kg/day |
| Sedentary | 0.8 g/kg |
| Low intensity exercise, recreational exercise | 0.8–1.0 g/kg |
| Regular moderate intensity exercise, moderate intensity endurance athletes | 1.2–1.5 g/kg |
| Ultra endurance athletes | 1.2–2.0 g/kg |
| Strength trained athletes | 1.6–2.0 g/kg |
Examples
Calculate the protein needs for a 170 pound sedentary man
170 lbs ÷ 2.2 = 77.27 kg
77.27 kg x 0.8 g/kg = 61.8 g/day
This 170 pound sedentary man requires approximately 62 grams of protein per day.
Calculate the protein requirement for a 150 pound strength trained woman.
150 lbs ÷ 2.2 = 68.18 kg
68.18 kg x 1.6 g/kg = 109 g/day
68.18 kg x 2.0 g/kg = 136.36 g/day
This 150 pound strength trained woman requires between 109-136 grams of protein per day.
Protein requirements can also be influenced by total energy intake and health status. Protein intake should be increased up to 2.0 g/kg per day during an energy deficit to help prevent loss of lean muscle mass (1). This applies to both athletes and nonathletes. Increased protein intakes may also be beneficial when recovering from injury or surgery as amino acids are required to repair and rebuild the damaged tissues. Additionally, vegetarians should increase their protein intake by approximately 10% compared to individuals who eat animal products.
Finally, older adults may benefit from slightly higher intakes of protein to help counteract sarcopenia or age related muscle loss. Sarcopenia can develop in adults in their 40s and can be mitigated by resistance training and increasing protein intake. Research suggests that as an individual ages, increasing protein intake to 1.1-1.2 g/kg per day may help prevent age-related sarcopenia (3).
Excessive Protein Intake
In the past, it was thought that high protein diets (intakes > 2.0 g/kg) would stress the kidneys and liver, especially if the source of the protein was from supplements. More current research has shown that this is not the case for athletes, and other individuals, with normal kidney function. In fact, long term protein intakes of > 3.0 g/kg do appear to be safe for healthy, active individuals. However, it is important to understand that if an individual has compromised kidney or liver function, consuming high amounts of protein may be harmful.
The main problems associated with high-protein intake are dehydration, low-carbohydrate intake, excessive caloric intake, and lack of variety. So consuming more than 3.0 g/kg of protein may not cause harm to your kidneys and liver but you may notice that you don’t have a variety of foods in your diet and you struggle to meet your carbohydrate needs because you’re prioritizing foods high in protein.
Large amounts of protein can result in dehydration because when protein intake exceeds the body’s ability to use it the amino acids are deaminated, and the carbon skeletons are used for energy production, glucose production, or converted to fat. The nitrogen that is removed is formed into urea and transported to the kidneys for excretion. This increases loss of body fluids in the form of urine. In addition, the breaking of peptide bonds during protein digestion requires water. Failure to meet fluid needs can result in dehydration which can jeopardize both the performance and health of an athlete. Luckily, this is a relatively easy problem to fix – drink adequate amounts of water.
Another potential problem with a high-protein diet is that it can come at the cost of an inadequate carbohydrate intake. Emphasis on high-protein foods may displace other nutritious, high-carbohydrate foods such as whole grains, fruits, and vegetables. These foods are also nutrient dense and provide vitamins, minerals, and fiber not found in animal products. In addition, this could result in low-muscle glycogen stores that can hurt the athletes’ ability to train and result in deteriorating performance.
Low Protein Intake
Although severe protein deficiency is rare in the developed world, it is a leading cause of death in children in many poor, underdeveloped countries. Kwashiorkor, a severe form of protein deficiency, affects millions of children worldwide. When it was first described in 1935, more than 90 percent of children with Kwashiorkor died. Although the associated mortality is slightly lower now, most children still die after the initiation of treatment. The name Kwashiorkor comes from a language in Ghana and means, “rejected one.” The syndrome was named because it occurred most commonly in children who had recently been weaned from the breast, usually because another child had just been born. Subsequently the child was fed watery porridge made from low-protein grains, which accounts for the low protein intake. Kwashiorkor is characterized by swelling (edema) of the feet and abdomen, poor skin health, stunted growth, low muscle mass, and liver malfunction. Recall that one of protein’s functional roles in the body is fluid balance. Diets extremely low in protein do not provide enough amino acids for the synthesis of albumin. One of the functions of albumin is to hold water in the blood vessels, so having lower concentrations of blood albumin results in water moving out of the blood vessels and into tissues, causing swelling. The primary symptoms of Kwashiorkor include not only swelling, but also diarrhea, fatigue, peeling skin, and irritability. Severe protein deficiency in addition to other micronutrient deficiencies, such as folate (vitamin B9), iodine, iron, and vitamin C all contribute to the many health manifestations of this syndrome.
Special Populations: Vegetarians
People who follow variations of the vegetarian diet and consume eggs and/or dairy products can meet their protein requirements by consuming adequate amounts of these foods. Vegetarians and vegans can also attain their recommended protein intakes if they give a little more attention to high-quality plant-based protein sources. However, when following a vegetarian diet, the amino acid lysine can be challenging to acquire. Grains, nuts, and seeds are lysine-poor foods, but tofu, soy, quinoa, and pistachios are all good sources of lysine. Following a vegetarian diet and getting the recommended protein intake is also made a little more difficult because the digestibility of plant-based protein sources is lower than the digestibility of animal-based protein.
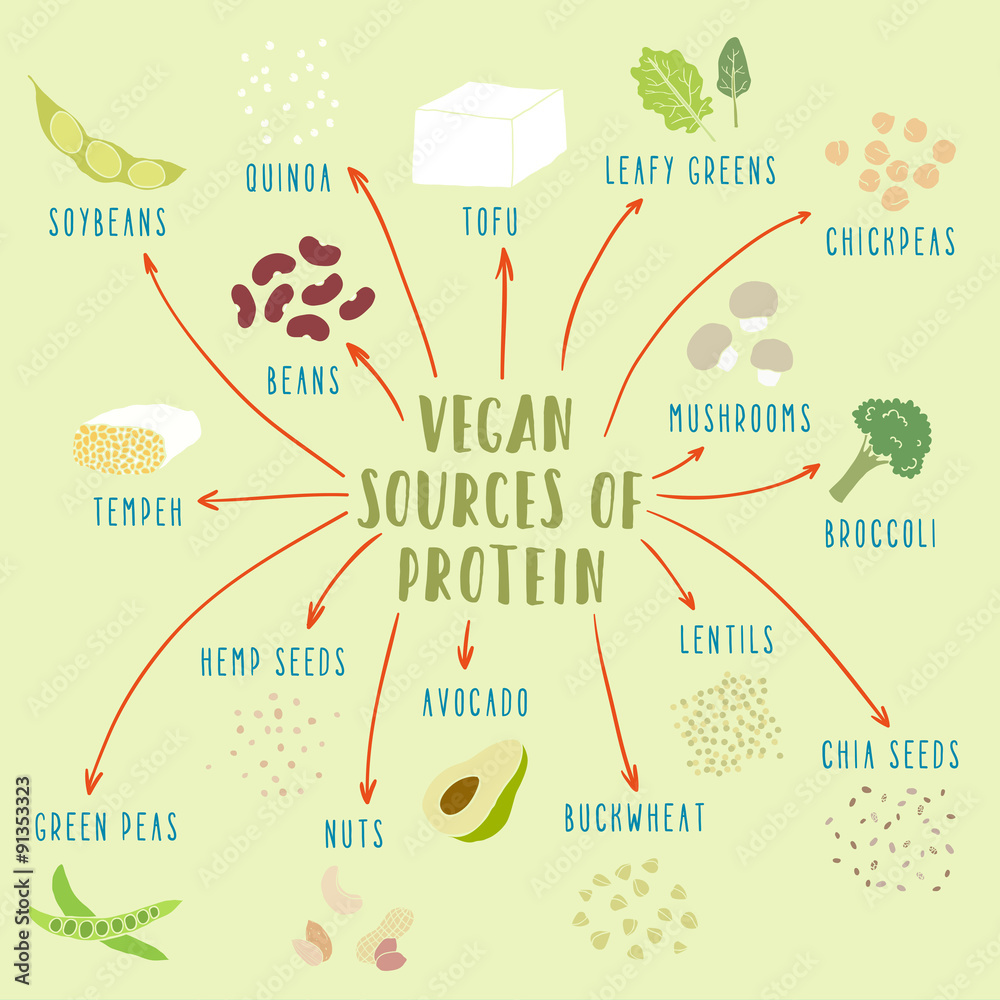
To account for the lower digestibility of plant proteins, it is recommended that vegetarians increase their protein intake by 10% compared to individuals who consume animal products. Figures 7.9 and 7.10 provide some suggestions for obtaining adequate protein intakes from plant based foods. Keep in mind that all of these foods contribute to overall protein intake, but they are not all sources of high quality plant protein.
Figure 7.9 Plant Based Sources of Protein
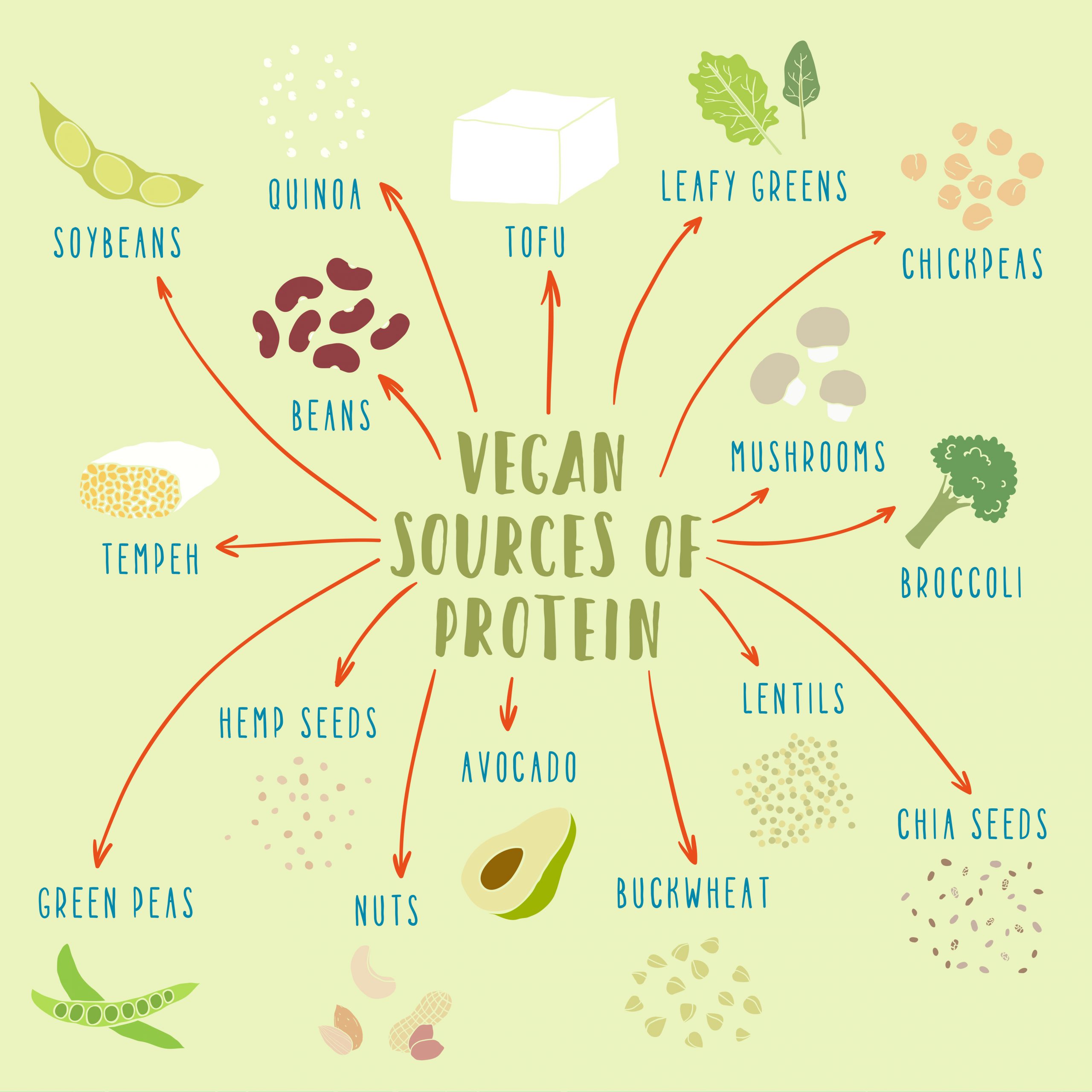
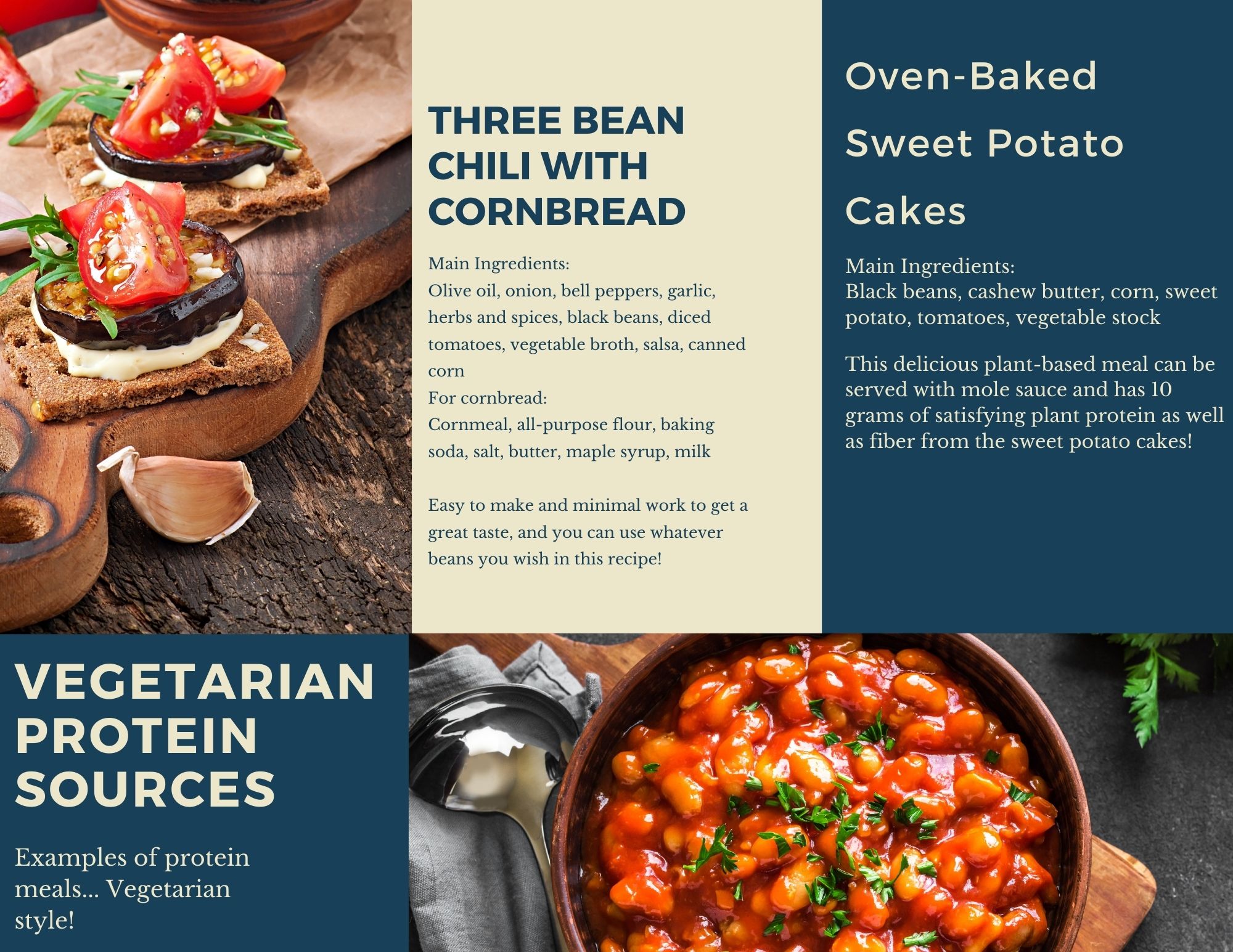
Figure 7.10 Ideas for Preparing High Protein Vegetarian Meals
Media Attributions
- Vegan Sources of Protein © Adobe Stock is licensed under a All Rights Reserved license
- Vegetarian Protein Sources 1 © Natalie Fox is licensed under a CC BY (Attribution) license

{kind=link}